
|
Total knee replacement is one of the most successful treatment interventions in modern medical practice. In this operation, the surface of the knee joint is replaced with metal components and a polyethylene insert is interposed, A large number of people have knee replacements and this page is intended to help the reader understand |




|


Arthritis of the knee
 The knee joint is a highly complex joint formed between the lower end of the thigh bone (femur) and the top end of the leg bone (tibia). The knee cap (patella) is located in front of the knee and articulates with the femur.
The knee joint is a highly complex joint formed between the lower end of the thigh bone (femur) and the top end of the leg bone (tibia). The knee cap (patella) is located in front of the knee and articulates with the femur.
The surface of femur and tibia, which form the knee joint, are lined with a smooth surface called the articular cartilage. Additionally, the knee has two crescent shaped cartilages called the menisci which are located between the femur and tibia and act as shock absorbers. There are four main ligaments in the knee – two cruciate and two collateral ligaments, which provide stability to the knee.
In arthritis, the articular cartilage becomes thin and wears out. This leads to knee stiffness, deformity and pain. Various conditions can affect the integrity of the articular cartilage. Most commonly, it is osteoarthritis (also called as osteoarthrosis), and other conditions include rheumatoid arthritis, arthritis following injury to the knee, and rarely tumours, rare inflammatory arthropathies, and infections.
Knee replacement is carried out to relieve pain from the degenerate joint.
Primary or revision knee replacement
The first time the natural knee joint is replaced is known as primary knee replacement. If further operations are required to change one of both components, it is called revision knee replacement. In a primary knee replacement, the lower end of femur is prepared to accept a femoral component and the upper end of the leg bone is prepared to accept the tibial component.
The two components are fixed into bone either with special acrylic bone cement, or by cementless fixation. In cementless fixation, the size and shape of the prosthesis accurately matches the prepared bone and the metal joint is coated with a special surface which encourages bone ingrowth into the metal, hence providing a firm fixation and long term stability. This special surface coating may be Hydroxy-apatite, or porous coating. Cemented fixation is used more commonly than cementless fixation in knee replacements.
The knee cap can be changed at the same time if required, but this is not routine.
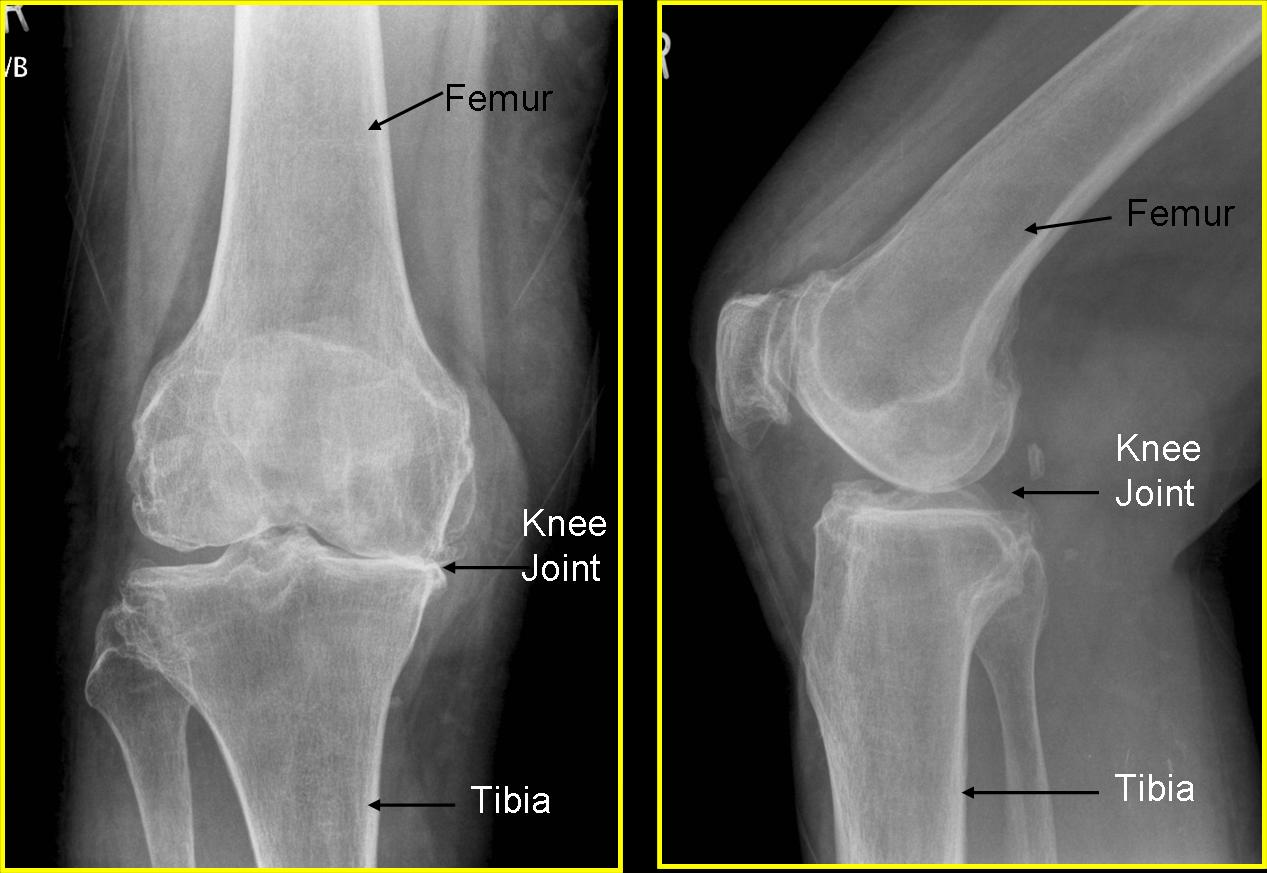
X rays showing arthritis of the knee. The space between the femur (thigh bone) and tibia (leg bone) is narrowed because of wearing of the joint surface
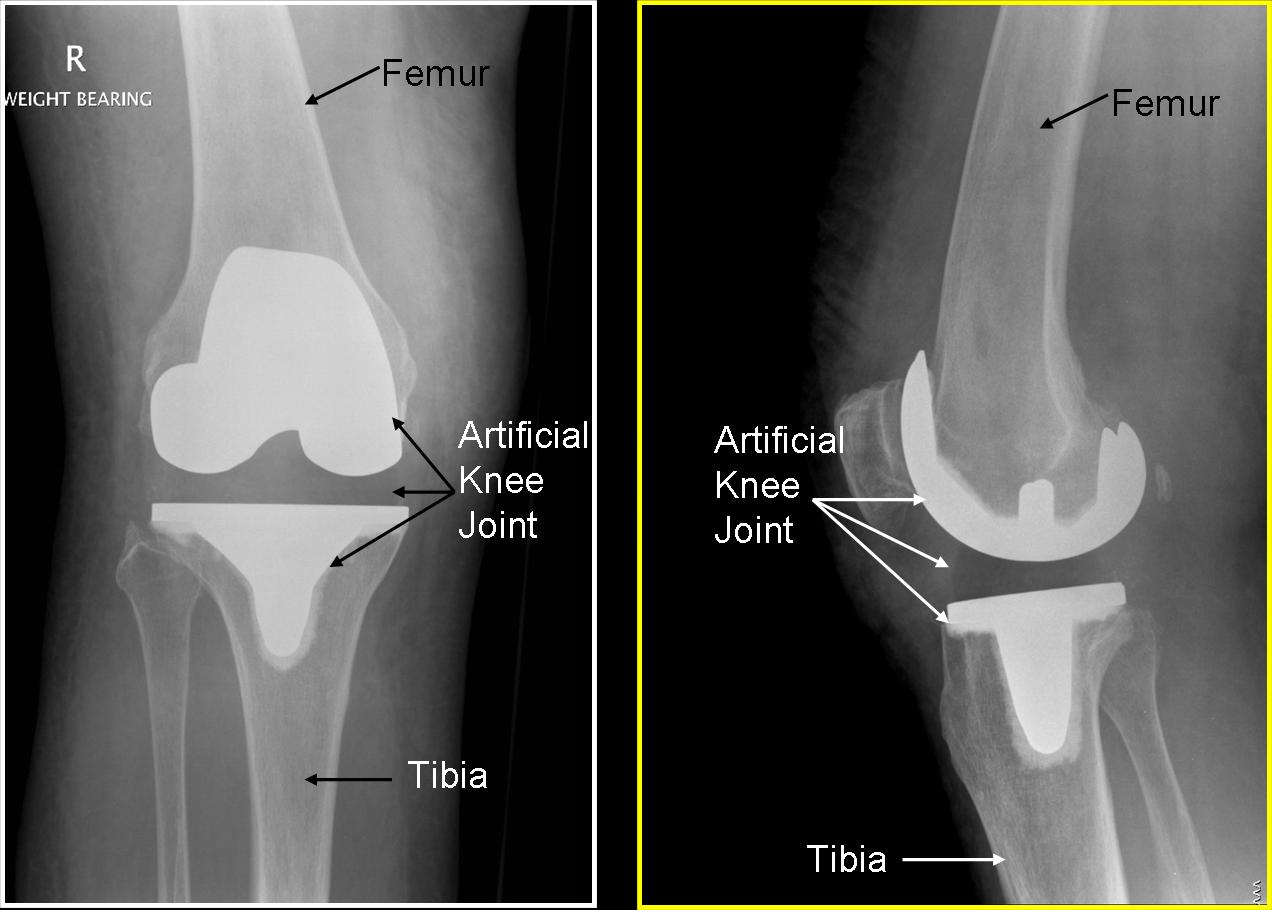
X rays after total knee replacement. The ends of the bone have been replaced with metal components and there is a plastic in the middle.
Computer guided knee replacement
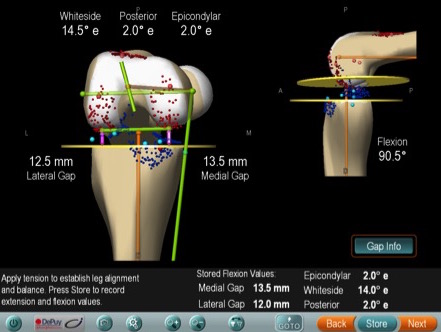
Computer navigation is used in knee replacement to achieve accurate placement of components. An infrared camera connected to computer gives the surgeon detailed data about surgical resection and soft tissue balancing. This information would not otherwise be available to the surgeon using conventional techniques. Additionally, it avoids insertion of alignment rods in the femur at the time of the operation, and is believed to reduce risk of fat embolism. The operating time is slightly longer with use of computer navigation, and this is because of time taken to set up and calibrate the computer. This technology is available in Cardiff with Mr Sanjeev Agarwal.

Personalised knee replacement
A new technique for doing knee replacement is by doing an MRI scan (Magnetic resonance Imaging) prior to the operation. On the basis of measurements in the scan, a special jig is prepared by the implant company. This fits accurately on the bone at the time of knee replacement and helps to achieve an accurate resection of bone. As with computer navigation surgery, the actual prosthesis used is the same as conventional technique. This technology is available in Cardiff with Mr Sanjeev Agarwal.


Gender specific knee replacement
Bearing in mind the differences in anatomy and dimensions of men and women knees, some knee replacements prosthesis have been designed specifically for women. These are supposed to provide a better fit, and hence better function. These special implants are available in Cardiff.
Materials for knee joint
The knee joint prosthesis has a femoral component made of cobalt – chrome. The tibial component is usually titanium or cobalt - chrome and has a plastic fixed to it which is a (UHMWPE) plastic liner. The patellar button is usually entirely made of UHMWPE and is cemented into the knee cap. In the x ray picture above, the two white parts seen on x rays in the artificial knee joint are the metallic parts, and the clear space in between the two parts is the plastic component.
The operation
 Knee replacement surgery is done under general anaesthetic or spinal anaesthetic. Spinal anaesthetic is used more commonly, as it is more comfortable for the patients and it helps in postoperative pain relief as well.
Knee replacement surgery is done under general anaesthetic or spinal anaesthetic. Spinal anaesthetic is used more commonly, as it is more comfortable for the patients and it helps in postoperative pain relief as well.
The operation is done with patients lying flat on the back. The incision is around 15cm in length, and is placed vertically on the front of the knee. The surgery takes 60 to 80 minutes. A thin plastic tube (drain) collects any postoperative bleeding in a small plastic bag. This blood is reinfused back. The drain is removed on the day after surgery. Pain relief is provided by a PCA (patient controlled analgesia) pump, whereby patients can press a button to control the amount of pain killers injected, as per requirement. There is a safety mechanism to prevent overdose.
Normal diet is resumed the day after surgery. Usual hospital stay is between 3 and 5 days.
Mobilisation is started on the day following surgery. Initially a Zimmer frame is used to help mobility and this quickly progresses to crutches and then sticks. By 6 to 8 weeks, most people are able to mobilise well, and some may take up to 3 months to regain best mobility. The physiotherapists will help regain the movements and the muscle strength in the knee following surgery, and a range of exercises is advised to achieve a speedy recovery.
Care after surgery
Following knee replacement, driving is not recommended for about 6 weeks. The insurance company should be informed about the knee replacement surgery. An automatic transmission car can be driven earlier after surgery to the left knee.
Heavy work and lifting heavy objects is not recommended after knee replacement. Running and contact sport are also not recommended. Golf is possible, as is doubles tennis. Riding a bicycle is allowed after 2 to 3 months. Walking is not restricted after knee replacement. Gardening is limited and many people may experience difficulty in kneeling down and / or squatting. Kneeling and Squatting are allowed after knee replacement but almost half the patients may find this difficult. If there was significant stiffness in the knee prior to surgery, it may be difficult to regain further movement after surgery. This means tying shoe laces and cutting toe nails may be difficult in these situations.
These are broad guidelines and individual circumstances dictate rehabilitation after total knee replacement. Through meticulous technique, improved implants and high standard of care, the outcome following knee surgery is better than ever before. I currently do over 200 hip and knee replacement operations annually, and in my experience, among patients with knee replacement surgery, infection rate is zero. Satisfaction rate is 95% and about 2% patients require redo operations at 4 year followup. These results have been possible through meticulous technique and ensuring the joint is adequately balanced and aligned. I have devised a new knee alignment device which wil ensure more accurate knee balancing in future.
If you have further questions, please contact us about your query, and I will be delighted to respond to any comments, questions or concerns.
Please, click on 'Risks of knee replacement surgery' to know more.